Annual Quality Account 2023-2024
Date published: 21 June 2024
Summary
Welcome to the East of England Ambulance Service NHS Trust Quality Account for 2023/24. This document has been approved by the Trust Board and is an accurate account of the level of quality of service provided to patients. In developing this Quality Account, we have set out a summary of achievements for 2023/24 and goals for 2024/25 as mandated within the regulatory guidance.
In this report
- Part One:
- Foreword and statement on quality from the Board
- Welcome to the East of England Ambulance Service NHS Trust
- Introducing the East of England Ambulance Service NHS Trust Quality Account and Improvements
- What is a Quality Account and what does it mean to EEAST and the people we serve?
- Our current quality position
- Care Quality Commission
- Department of Health Core Quality Indicators
- NHS number and General Medical Practice Code validity
- Clinical coding error rate
- Data quality
- Data Security Protection Toolkit
- Statement of accountability
- Part Two:
- How have we prioritised our quality improvement initiatives
- Priority one: Patient safety
- Priority two: Clinical effectiveness
- Priority three: Patient experience
- Part three:
- Progress on the quality account priorities 2023/24
- Performance of the Trust against mandated quality metrics
- Achievements against local priorities set for 2023/24
- Clinical audit
- Participation in research
- Patient safety incidents
- Serious incidents
- When things go wrong
- Duty of Candour
- National Patient Safety Alerts
- Patient experience and feedback
- Patient and public involvement
- Raising concerns and Freedom to Speak Up
- Working with our local communities
- Commissioning for Quality and Innovation (CQuIN)
- Quality Governance Committee Assurance
- Statements from stakeholders
- Acronym
What is a Quality Account and what does it mean to EEAST and the people we serve?
A Quality Account is a mandatory report about the quality of services an NHS healthcare trust provides and is required to be completed in line with the Health and Social Care Act 2012.
Quality reports and accounts are set against the framework of three overlapping key themes, patient safety, clinical effectiveness and patient experience, which can be used to define quality of care.
The content is defined by NHS England and includes outcome results against specific indicators under five headings:
- Preventing people from dying prematurely.
- Enhancing quality of life for people with long term conditions.
- Helping people to recover from episodes of ill health or following injury.
- Ensuring that people have a positive experience of care.
- Treating and caring for people in a safe environment and protecting them from avoidable harm.
Data Security Protection Toolkit
Data Security Protection Toolkit (DSPT) is an online self-assessment tool that allows organisations to measure their performance against the National Data Guardian’s ten data security standards. All organisations that have access to NHS patient data and systems must use this toolkit to provide assurance that they are practising good data security and that personal information is handled correctly. The DSPT also provides the Trust with a means of reporting data breaches and data security incidents.
Following the delayed national submissions in previous years, the 2023/24 assessment submissions continued to have the deadlines of February 2024 for the baseline submission and June 2024 for the final submission.
The Trust submitted the baseline assessment on the 29 February 2024 where 88 of the mandatory evidence items were met, this included a mandatory item which NHS England requested an update on. The Information Governance team hold frequent meetings which concentrate on gaps where evidence is needed to complete a mandatory item.
The Trust has currently completed 91 of the 108 mandatory evidence items, with 7 out of 34 assertions confirmed and are working towards completing the final standards by the 30 June submission. Progress against these outstanding areas will be monitored through our Information Governance Group and assurance provided to the Trust Board through our Audit Committee. The Trust will strive to meet all the mandatory items to be assessed as Standards Met, which was achieved last year for the 2022/23 toolkit.
For the 2024/25 toolkit, NHS England have announced the DSPT will be aligned with the Cyber Assessment Framework (CAF), where there will be 47 contributing outcomes, which the Trust will need to provide evidence and provide answers of “not achieved,” “partially achieved” and “achieved”. Profiles for organisations have been built with a minimum requirement set for organisations to work towards and achieve Standards Met. This will be released in September 2024.
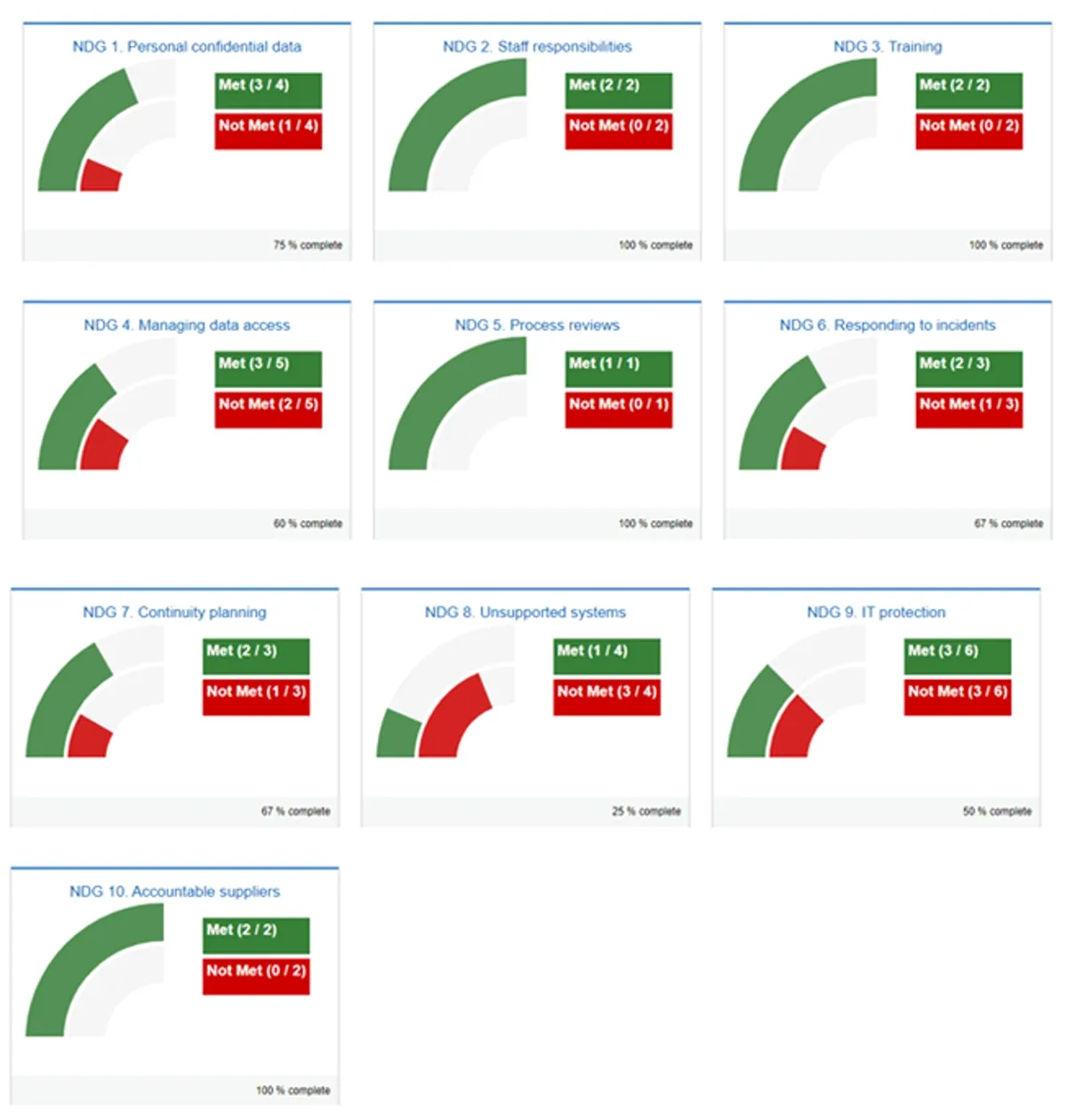
| National Data Guardian | Met | Not met |
|---|---|---|
| 1. Personal confidential data | 3/4 | 1/4 |
| 2. Staff responsibilities | 2/2 | 0/2 |
| 3. Training | 2/2 | 0/2 |
| 4. Managing data access | 3/5 | 2/5 |
| 5. Process reviews | 1/1 | 0/1 |
| 6. Responding to incidents | 2/3 | 1/3 |
| 7. Continuity planning | 2/3 | 1/3 |
| 8. Unsupported systems | 1/4 | 3/4 |
| 9. IT protection | 3/6 | 3/6 |
| 10. Accountable suppliers | 2/2 | 0/2 |
Performance of the Trust against mandated quality metrics
Response Times
Ambulance services are monitored against response times for a Category 1 – 4 system (determined by clinical condition/emergency), with varying response times for each category. The table below summarises the Trust’s performance against the national response time standards for 2023/24 and shows that there was improvement in all categories when compared to the previous year.
Published further information for all ambulance services can be found here: www.england.nhs.uk/statistics and more detailed information relating to EEAST can be found within our Annual Report.
| Category | Definition | National standard | Average EEAST Performance (hh:mm:ss) 2022/23 and 2023/24 |
|---|---|---|---|
| C1 | Immediately life-threatening injuries and illnesses. | 7 minutes mean response time | 00:10:25 and 00:09:03 |
| 15 minutes 90th centile response time | 00:19:30 and 00:17:04 | ||
| C1T | Immediately life-threatening injuries and illnesses where the patient is transported to hospital. | 7 minutes mean response time | 00:13:49 and 00:11:55 |
| 15 minutes 90th centile response time | 00:25:05 and 00:21:53 | ||
| C2 | Emergency. | 18 minutes mean response time | 01:06:56 and 00:43:51 |
| 40 minutes 90th centile response time | 02:28:36 and 01:35:56 | ||
| C3 | Urgent calls and in some instances where patients may be treated in-situ (e.g., their own home) or referred to a different pathway of care. | 120 minutes (2 hours) 90th centile response time | 07:36:23 and 05:03:57 |
| C4 | Less urgent. In some instances, patients may be given advice over the phone or referred to another service such as a GP or pharmacist. | 180 minutes (3 hours) 90th centile response time | 11:40:43 and 08:49:30 |
In September 2023, EEAST implemented the national principles of C2 segmentation. This is to ensure that we classify the risk within the C2 category that accounts for over 60% of ambulance workload we receive. EEAST has managed C2 calls via Hear and Treat for many years, so the focus has been on increasing staffing and improving processes. Since the process went live, EEAST has increased the number of C2s receiving an appropriate Hear and Treat outcome from 4% to 6%. The impact of C2 response times is still being evaluated.
The increased demand on our services and the handover delays experienced at hospitals within the year has also contributed to the delays seen in attending our patients. To improve our performance, we have worked hard with our system partners and implemented a number of actions such as, co-horting of patients at hospitals to release ambulance clinicians back into the community, alongside moving calls to community providers via the Access to Stack process which is now embedded and consistent. The Trust routinely moves across 4000 calls a month of which 70% are accepted by the community providers. This allows the patient to receive the most appropriate service when they have dialled 999. There is continued work with establishing the six Unscheduled Care Coordination Hubs to deliver the appropriate care to patients.
All calls (with some specific exceptions) now go into the Trust’s Clinical Assessment Service (CAS) stack once received. This ensures that we can optimize the potential to manage the patient in a different way therefore protecting the response to our most ill patients.
The CAS team has been expanded and there are currently 24 validators who have moved to remote working from our Emergency Operations Centres (EOCs) as well as another five who are requesting a hybrid arrangement and are awaiting hardware. We have successfully recruited our first trained and qualified externally recruited validator with a further five due to be inducted and signed off during April. We plan for another five externally recruited staff to be trained during May.
We have also successfully recruited five new clinical workforce managers who are progressing through recruitment processes with an aim to interview four more before the end of quarter 1.
This new key role has been implemented to provide and embed a supportive, motivational, and compassionate leadership culture across the EOC, leading and supporting the CAS teams to deliver the best possible patient care.
The anticipation is that we can become more robust with individual performance and offer a more supportive approach to improving our compliance with clinical targets.
The Trust have introduced the first digital solution using artificial intelligence (AI) to help with identifying and automating a direct referral to community services concerning low acuity falls.
Currently, the Trust, through clinical navigation, manually identify and transfer calls to other health care providers, a system known as ‘access to the stack’. With oversight of the Trust Medical Director and the Senior Clinical Managers within the Emergency Operations Centre, the digital team have successfully created and currently piloting using an automated AI bot to identify, select and transfer low acuity falls responses after the call has passed through the call handling process. The pilot is being monitored with clinical oversight and if successful, the Trust are looking at expanding the call identification to other low acuity code sets.
Heart attack care
Heart disease continues to be one of the UK’s leading causes of death and is the most common cause of premature death, responsible for around 66,000 deaths in the UK each year.
As many as 100,000 hospital admissions each year are due to heart attacks. Because of the life-threatening risk with a heart attack, providing patients with a pre-hospital assessment for a STEMI and administering an appropriate care bundle means a significant improvement on patient outcomes, thereby supporting the NHS to reduce the number of patients dying prematurely and to help people to recover from episodes of ill-health or following injury.
STEMI care bundle
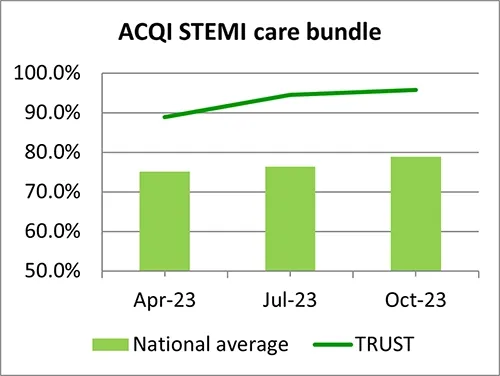
The mandatory quality indicator for ambulance services relating to this topic is the provision of an appropriate care bundle; recording of two pain scores, giving aspirin to break down the clot, giving glyceryl trinitrate (GTN) to dilate the coronary arteries and providing pain relief. The patient care record is audited against all of these criteria and deemed to be either compliant or non-complaint.
The data is reported on quarterly within the year and the table below shows our result against the national average and the best and worst scores achieved by ambulance services within England.
To provide a robust comparison, the table shows our achievement against the average and upper and lower compliance levels for ambulance trusts that have been published to date (April - October 2023). The graph demonstrates our performance against the national average for each quarter (April - November 2023), both demonstrating that the Trust is well above the national average for each quarter within the year.
 |
National data (April to October 2023)
| Heart attack care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| STEMI care bundle | 76.8% | 94.9 % | 57.1% | 93.0% |
EEAST was the second highest performing Trust for this care bundle achieving 16.2% above the national average for this period. April - October 2023
Patients conveyed to a Primary Percutaneous Coronary Intervention (PPCI) Centre
Although the time it takes to transport a STEMI patient to a specialist Primary Percutaneous Coronary Intervention (PPCI) treatment centre is not a quality metric for the Quality Account, we report our achievement on a month-by-month basis to both NHSE and our commissioners.
This ACQI contains two joint indicators for ambulance trusts and these centres both of which are measured in hours and minutes.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April - November 2023). It should be noted that the lower score is the best performing score within these outcomes.
Latest data available April - November 2023 (hh:mm)
| Heart attack care | National average | Upper | Lower | EEAST performance |
|---|---|---|---|---|
| Mean average time from call to catheter insertion for angiography | 02:27 | 03:00 | 02:13 | 02:32 |
| 90th centile time from call to catheter insertion for angiography | 03:26 | 04:06 | 03:08 | 03:26 |
Although meeting the national average for the 90th centile, EEAST performed just outside the national average for the mean.
However as demonstrated in the previous section, all patients received excellent care, with EEAST consistently achieving high compliance for the STEMI care bundle and being the second highest performing trust within the year.
Next steps:
As well as continually being monitored through the national ACQI programme, one of the Trust’s priorities for the year ahead is to reduce our response times to Category 2 calls which includes STEMI patients. This will be supplemented by a local priority for reducing the time spent on scene with these patients which will be monitored through a quarterly audit.
Stroke care
Stroke is a type of cerebrovascular disease, which is one of the leading causes of death in the UK accounting for approximately 75% of deaths from cerebrovascular diseases.
Face-arms-speech-time (FAST) is a simple test to help people recognise the signs of stroke and understand the importance of emergency treatment. The faster a stroke patient receives treatment (the care bundle), the better the chances are of surviving and reducing long-term disability.
Stroke diagnosis bundle
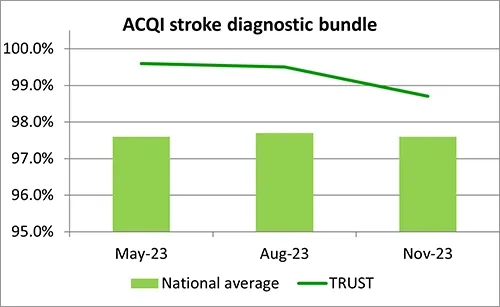
This quality metric relates to the percentage of suspected stroke patients (assessed face to face) who receive an appropriate assessment; recording of blood pressure (BP), FAST test and blood sugar levels (BM) the outcomes of which can be used to diagnose a possible stroke. As for heart attacks, the patient care record is audited against all of these criteria and must meet them all for the overall bundle to be compliant.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April – November 2023).
 |
National data – April - November 2023
| Stroke care | National average | Highest score | Lowest score | EEAST |
|---|---|---|---|---|
| Stroke Diagnostic Bundle | 97.6% | 99.6% | 89.1% | 99.3% |
EEAST was the second highest performing trust for this bundle achieving 100% in 2 out of the three reporting months. April - November 2023
Next steps:
In May 2024, NHS England advised ambulance trusts that this ACQI was being removed from the annual programme with immediate effect. However data will still be collected and reported on in relation to stroke timeliness (please see next page).
Stroke Timeliness
Patients who are cared for in a defined stroke unit with organised stroke services are more likely to survive, have fewer complications, and return home and regain independence quicker than patients on a general medical ward.
Although the time it takes to convey a stroke patient to hospital is not a quality metric for the Quality Account, we report our achievement on a month-by-month basis to both NHSE and our commissioners. Our performance is assessed monthly against three indicators for this ACQI: the mean average, median and 90th centile times from call to hospital arrival.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April – November 2023). The Lower level relates to the best performing trust for this outcome.
It should be noted that not all strokes are identified at the time of call due to the information provided to the call taker, or the patient may deteriorate before or after the crew arrive.
National data – April – November 2023 (hh:mm)
| Stroke care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| Mean average time from call to hospital arrival | 01:35 | 01:52 | 01:21 | 01:35 |
| Median time from call to hospital arrival | 01:21 | 01:34 | 01:12 | 01:23 |
| 90th centile time from call to hospital arrival | 02:27 | 02:57 | 02:04 | 02:25 |
Although on average EEAST performed just outside the national average for the median indicator for this time period, it matched against the mean and performed better in relation to the 90th centile.
However as demonstrated in the previous section and as per the STEMI ACQI, all patients received excellent care, with EEAST consistently achieving high compliance for this ACQI and being the second highest performing trust within the year.
Next steps:
As well as continuing to be monitored through the national ACQI programme, one of the Trust’s priorities for the year ahead is to reduce our response times to Category 2 calls which includes stroke patients. This will be supplemented by a local priority for reducing the time spent on scene with these patients which will be monitored through a quarterly audit.
Cardiac arrest care
A cardiac arrest occurs when the heart suddenly stops pumping blood around the body. Someone who is having a cardiac arrest will suddenly lose consciousness and will stop breathing or stop breathing normally. Unless immediately treated by cardio-pulmonary resuscitation (CPR) and early defibrillation, this always leads to death within minutes. It is, however, possible to survive and recover from a cardiac arrest if you get the right treatment quickly. Around two-thirds of cardiac arrests outside of hospital happen in the home, but nearly half of those that occur in public are witnessed by bystanders. With each minute that passes in cardiac arrest before defibrillation, chances of survival are reduced by about 10%.
This year we set out to improve the Trust’s outcomes from cardiac arrest and work towards an increase in Return of Spontaneous Circulation (ROSC) and ‘survival to discharge’ figures.
Although the indicators displayed in the table below are not quality metrics for the Quality Account, we report our achievement on a month-by-month basis to both NHS England and our commissioners, the exception being the post-ROSC care bundle which is a quarterly requirement.
The post-ROSC care bundle contains six components, the recording and administration of: 12 lead ECG; blood glucose; end tidal CO2; oxygen; systolic blood pressure, and saline fluids for all patients who achieve a ROSC on scene which continues to hospital. Patients who had suffered a traumatic cardiac arrest, were successfully resuscitated before the arrival of ambulance staff or were aged less than 18 years are not included.
The table below shows our result against the national average and the upper and lower levels achieved by ambulance services within England for data published to date (April – November 2023).
National data, April - November 2023
| Cardiac arrest care | National average | Upper | Lower | EEAST |
|---|---|---|---|---|
| Return of Spontaneous Circulation (pulse) at hospital – All patients | 28.9% | 32.4% | 25.8% | 29.1% |
| Return of Spontaneous Circulation (pulse) at hospital – Utstein patients | 51.8% | 65.4% | 46.1% | 55.5% |
| Survival to Discharge – All patients | 9.7% | 11.6% | 7.1% | 9.6% |
| Survival to discharge – Utstein patients | 30.2% | 41.8% | 23.3% | 35.7% |
| Post-ROSC care bundle | 75.9% | 97.4% | 62.9% | 95.2% |
With the exception of 30-day survival (all patients group), EEAST is performing above the national average for all cardiac arrest related indicators. It was also the second highest performing average compliance for the Post-ROSC care bundle and 19.3% better than the national average for the time period.
It should be noted that not all ambulance trusts submitted full data, so these outcomes must be used with caution.
Next steps:
This will continue to be monitored through the national ACQI programme. Successful outcomes from cardiac arrests are, in part, due to actions taken by acute organisations following arrival at hospital as well as early access to treatment and intervention as well. As our response times improve, so should our rates of ROSC and survival.
Patient safety incidents
A patient safety incident is defined as any unintended or unexpected incident which could have or did lead to harm for one or more patients receiving NHS care. This includes:
- incidents that caused no harm or minimal harm
- incidents with a more serious outcome
- prevented patient safety incidents (known as ‘near misses’).
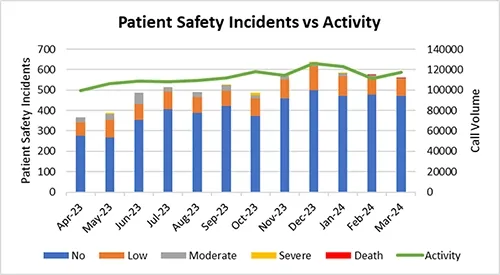
The number of incidents reported by staff during 2023/24 demonstrates a good culture of reporting and being open and honest. Where a near miss has happened, proactive steps can be taken to reduce the risk going forwards and to maintain a learning from incidents culture. The number of patient safety incidents relating to delays has decreased since 2022/23.
The chart below shows the number of patient safety incidents reported versus our activity during the year.
Previously all NHS organisations had a responsibility to report any safety incidents relating to patients through the National Reporting and Learning Service (NRLS). However, within the last year, this was superseded by the Learning from Patient Safety Events (LFPSE) which EEAST implemented on 01 October 2023. More information on LFPSE can be found in the next section.
Prior to the implementation of the Patient Safety Incident Response Framework (PSIRF) EEAST reported on the level of harm they directly caused in relation to individual incidents. Since the implementation of PSIRF in October 2024, the parameters to which levels of harm are reported has been updated in line with Learning From Patient Safety Events (LFPSE) guidance to reflect how EEAST may have contributed towards harm.
A requirement within the Quality Account requirements is for each trust to provide a comparison of their patient safety incidents reported to NRLS against the national average for similar services.
However, with this process moving to the new reporting platform, reports have been paused and no data had been published for 2023/24 at the time of writing this document.
Patient experience and feedback
Although not mandated to report on patient experience, as a Trust we feel that it is really important to tell people how we are continually improving our services as a result of our patients’ experiences and feedback. Patients are at the heart of everything we do, and as such we believe that patient voice should be a key driver in the way that we improve our services. The following pages provide information on what our patients and their families have told us through complaints, concerns, compliments and surveys, what steps we have taken to improve and how we intend to improve further in the future.
The Patient Experience Team co-ordinate complaints, concerns, compliments and comments for the Trust, in line with the NHS Complaints Regulations 2009 and local policy. All feedback, both positive and negative, is managed and recorded by the department. Communication with patients or their families is maintained throughout the process and they are provided with a response to their feedback, with a focus on resolving complaints and identifying learning at the earliest opportunity.
Compliments
Compliments always far outweigh the number of complaints received, and in 2023/24, 3,634 compliments were reported to the Trust, which equated to an average of 302 per month (a significant increase on the previous year’s average of 225 per month) compared to 495 complaints received. Compliments are reported to the Trust board and the individual colleague and are recorded on the staff member’s personnel file. This year we have started looking at themes from compliments to help us learn from excellence, and the common themes include kindness and compassion, calmness and reassurance, professionalism and good clinical assessment and treatment, with many compliments described as lifesaving.
| Apr-23 | May-23 | Jun-23 | Jul-23 | Aug-23 | Sep-23 | Oct-23 | Nov-23 | Dec-23 | Jan-24 | Feb-24 | Mar-24 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Compliment | 203 | 235 | 308 | 328 | 320 | 264 | 283 | 297 | 292 | 324 | 351 | 365 |
| Concern | 40 | 49 | 46 | 55 | 61 | 35 | 42 | 57 | 28 | 57 | 48 | 36 |
| Complaint | 39 | 31 | 42 | 39 | 29 | 38 | 41 | 58 | 45 | 36 | 44 | 53 |
Complaints
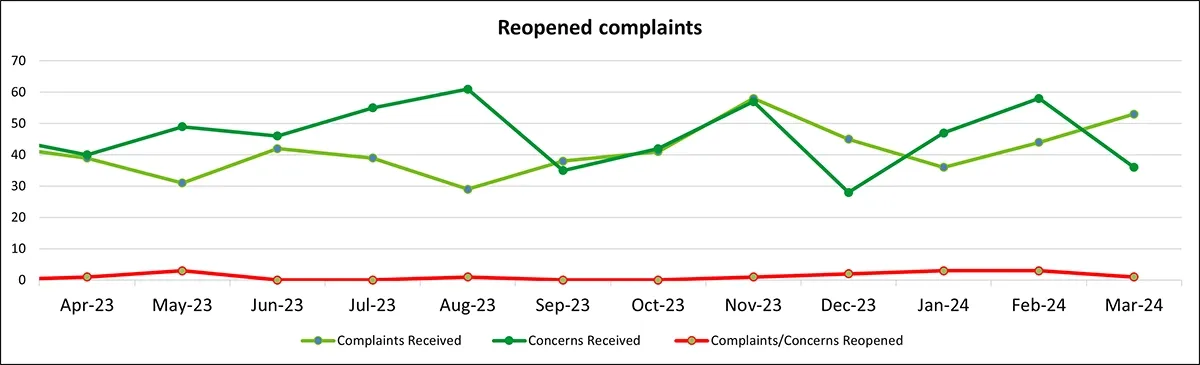
As a Trust we closely monitor the numbers and themes of complaints that we receive and use this learning to support service improvement. During 2023/24 complaints and concerns arose from 0.06% of our contacts with patients which is an improvement of 0.1% on the previous year. All complaints and concerns which cannot be resolved under early resolution receive a local investigation and depending on the nature of the complaint or concern, may also be reviewed by the patient safety team. Complainants are supported through the process of raising a complaint and investigation by our patient experience coordinators, and upon receiving a written response, face to face meetings are arranged where complainants require further support.
The number of re-opened complaints remains very low, meaning complainants are usually satisfied that our responses have addressed and, where able, resolved their questions and concerns.
The biggest themes from complaints and concerns were delay (these mostly related to delays in the patient transport service, with only 22% of delay complaints relating to emergency operations centres and emergency services), transport and driving (which again mostly related to the patient transport service, which accounted for 94% of these), and clinical assessment and treatment (of which 85.9% were for emergency operations centres and emergency services). These themes reflect the improvements in emergency ambulance attendance times achieved via the Trust’s delay action plan, however a significant number of the clinical assessment and treatment complaints relate to either no sends or treatment at home under this same plan, suggesting that some patients have not felt confident that the alternative care pathways offered were right for them. These complaint themes also reflect a challenging year for the patient transport service, with some of our services delivering journey volumes more than the contracted levels.
You said, we did
As a Trust we recognise the importance of learning when things have not gone as well as we would have liked. Through feedback received from our patients, carers and relatives we have an opportunity to put things right and to prevent future recurrences. All our teams at EEAST are passionate about improving the services that we provide to our patients and the public.
The following case studies are just two examples of some of the learning that has been taken forwards by the Trust over the last year.
| You said | What we did | What this means |
|---|---|---|
| 1. We received complaints and feedback from patients using the patient transport service who had either struggled to ascend the sidestep to our new ambulances, or who had fallen using this step. | This feedback was passed to the patient safety team to review the safety impact of this for patients. Initially whilst this concern was investigated, the Patient Transport Service were advised not to use the sidestep in order to prevent further injury. The patient safety team, the health and safety team, fleet and the patient transport service worked together to retrofit handrails to make it easier and safer to use these steps. | Patient feedback has directly influenced the way that the patient transport team support patients to enter the ambulances. The ambulances now have more support to allow patients to enter them more safely and to reduce the risk of any future injuries. |
| 2. Feedback was received from two members of the public about driving standards around horses. They were concerned that the use of sirens near the horses could have caused a further accident. | The initial incident was reviewed, and the driver involved was supported to reflect on his actions. The information was passed onto the driver training unit and professional standards team, who contacted the complainants to gain a better understanding of their concerns and the situation they described. An article was written and placed in the safety matters newsletter to highlight the issues of driving under blue light conditions around horses, and to educate drivers on how to minimise risk when passing driving in close proximity to horses. | Drivers of our ambulances will be more aware of the potential dangers of passing horses whilst driving under blue light conditions. They will also be more aware of how to reduce any risks to the horses and their riders. The complainants in question also have increased confidence in our response to feedback and commitment to the safety of all road users. |
Parliamentary and Health Service Ombudsman (PHSO)
Although most complaints are successfully resolved through the Trust’s complaints process, complainants are able to refer their complaint to the Parliamentary and Health Services Ombudsman (PHSO) for an independent review. This happens if a complainant feels that their complaint has not been resolved and the Trust has exhausted all avenues of resolution. This provides complainants with an impartial, independent review of their complaint and gives clear guidance to the Trust on how to improve our investigations and responses.
In 2023/2024 the Trust was notified of eight cases which had been referred to the PHSO by complainants. Of these, so far none have been opened for investigation; four have been closed following initial review by PHSO and four remain in the initial review phase. In addition, there are three open investigations dating from 2022/2023. We have received initial feedback for one of these, and the PHSO have indicated that on current information this is unlikely to be upheld. The PHSO has a significant backlog in respect of investigations, and as such we are seeing cases remain in the initial review and investigation phase for extended amounts of time.
The PHSO continued to undertake training and develop processes in line with the PHSO NHS Complaints Standard Framework. The team and the Trust are largely working to this framework, however there are some changes required for 2024/2025 in terms of reporting and training.
Patient surveys
As stated within a previous section, the Trust has a comprehensive annual patient survey programme which includes continuous surveys for the emergency service (ES), Clinical Assessment Service (CAS) and the patient transport service (PTS). Planned survey projects undertaken will vary in line with the Trust’s priorities and strategies. These projects are often co-produced with experts by experience to ensure people and our community are treated as equal partners in service design, development, and evaluation.
Patient surveys are signposted using various methods, including the Trust’s social media channels, patient information cards and invitation to feedback letters, which are posted to random samples of ES and PTS patients every month. During 2023/24, Short Message Service (SMS) survey signposting commenced for PTS patients across the region. Approximately half of the PTS survey submissions received during year have been as a result of the SMS signposting.
Listening to the patient voice enables the Trust to identify, not only what is working well, but also to highlight areas for learning and service improvement. Feedback received through surveys is monitored and triangulated with the themes identified through complaints, patient engagement, and patient safety to ensure appropriate governance, learning, and to improve patient experience and outcomes.
All patient surveys include the Friends and Family Test (FFT) question, ‘Overall, how was your experience of our service?’ as good practice. The FFT is a method of calculating the overall satisfaction of the patient and is used as a benchmark across the Trust. The FFT result is calculated by dividing the proportion of ‘very good’ and ‘good’ responses (numerator), by the overall number of responses (denominator). The FFT is a national directive, and the Trust is required to provide all PTS patients with the opportunity to respond to the FFT question, with results reported to NHS England each month.
Outcomes from this and the previous year’s rolling overall satisfaction results for the ES/CAS and PTS continuous survey can be found in the table below. This shows a slight reduction for all services which is an indicator of the pressures that we experienced during the year.
Overall Satisfaction (Friends and Family Test)
| Trust Patient Experience Results: April 2022 to March 2023 | Number of patients: 2022/23 | Overall Satisfaction: 2022/23 | Number of patients: 2023/24 | Overall Satisfaction: 2023/24 |
|---|---|---|---|---|
| Emergency Services / Clinical Assessment Service | 827/909 | 91.0% | 737/826 | 89.2% |
| Patient Transport Service | 405/466 | 86.9% | 1057/1252 | 84.4% |
| All Services | 1232/1375 | 89.6% | 1794/2078 | 86.3% |
Survey projects
The following provides further information on each of the surveys undertaken throughout the year.
Easy-Read
During 2022/23, an EasyRead survey was co-produced with the D.R.A.G.O.N.S at the Norfolk and Norwich SEND Association (NANSA) – highlighting the importance of co-production and working with experts by experience as equal partners. Since April 2023, the survey has been available for ES and PTS patients to share their experience relating to the service received. Feedback has generally been positive (overall satisfaction: 93.9%); the main area of dissatisfaction has related to delays/non-attendance, which has been shared as part of the wider system review.
Safeguarding
The safeguarding survey has continued throughout 2023/24, with the aim being to obtain feedback from patients who had consented to a safeguarding referral (e.g., mental health services, falls team, GP, local authorities and the Fire and Rescue Service). Overall satisfaction with the service received has been high (95.9%), with patients generally felt included to at least ‘some extent’ (88.1%) in discussions relating to their referral and support required.
Dissatisfaction has mostly related to clinical treatment/assessment and delays, with such feedback discussed as part of the Safeguarding Group.
Maternity
The maternity survey remained available throughout 2023/24, enabling patients to provide feedback following their maternity related 999-emergency call. Satisfaction has remained high (95.6%), with patients mostly reporting a positive experience of the service. Ambulance service staff continue to be rated as ‘good’ or ‘excellent,’ with patients also reporting that they were treated with dignity and respect.
Feedback has also related to the need for additional paramedic obstetric training, with a call for instructions provided by call handlers to be reviewed. This feedback was shared with the Trust’s relevant clinical lead and specialist midwife for consideration going forward.
No-Send
During 2023/24, a further mailout of the no-send survey was undertaken to capture feedback from category 2 to category 5 patients who had not received an ambulance response due to unprecedented demand. Overall satisfaction with the service received was poor, however, patients generally understood the instructions provided by the emergency call handler and 93.5% had followed the advice given.
Dissatisfaction predominantly related to ambulance non-attendance, and the lack of early communication to advise that an ambulance response would not be dispatched. The feedback received in relation to non-attendance/delays has been included as part of the wider work relating to the current urgent and emergency care situation.
Skin Tear
The skin tear treatment survey has continued throughout 2023/24, with the aim to obtain feedback from patients who had received skin tear wound treatment. All patients rated the service as ‘good’ or ‘very good,’ with patients treated at home generally pleased (93.3%) to have received out of hospital care and avoided the need for hospital conveyance.
The main area of dissatisfaction has continued to relate to ambulance delays, which has been included as part of the wider system review. Additional feedback related to the need for wound dressing guidance/instructions and follow up. The relevant clinical lead is leading a communications drive for Trust staff in relation to skin tear injuries and treatment.
Mental health
During 2023/24, two quarterly mental health surveys have continued to obtain feedback from patients who have contacted the service in relation to a mental health crisis. These survey projects include a young person Instagram survey (designed in collaboration with the Youth in Mind Group at the Mancroft Advice Project) and an online mental health survey (co-produced with the SUN Network) which was trialled as a social media poll survey during Q3.
Survey feedback continues to demonstrate satisfaction with the service received from the Trust (generally between ‘good’ and ‘very good’ on the sliding scale), although some patients have reported not feeling listened to or understood by the emergency call handler. Survey feedback continues to highlight the need for improved mental health service support and signposting prior to patients reaching crisis point. The survey results have been shared widely to ensure 360 feedback, working with commissioners, partner organisations and experts by experience to ensure system wide learning and improvements to the service provided to patients.
Going forward, call handler engagement sessions and training are planned. In addition, lists of area specific mental health services/support will continue to be shared, with plans in place to produce to a video relating to the 999 call-handling process and algorithm.
Stroke video triage
During 2023/24, two stroke video triage survey mailouts have been undertaken for patients who received a pre-hospital stroke video triage assessment within the West Essex and Peterborough areas. Patients have mostly felt satisfied with the service received (91.3%) and pleased to have received an assessment by way of video triage. However, some patients were unaware that an assessment had been undertaken using this virtual method – prompting the need for improved communication going forward.
The feedback received has highlighted the benefits of utilising technology to improve patient experience and outcomes, in line with the NHS Long Term Plan.
Next steps
The Trust is committed to developing its patient experience and engagement activity and continually explores new methods to obtain feedback and to ensure the voice of patients within seldom heard groups are heard. Co-production and working with experts by experience will continue, placing our patients and communities at the heart – particularly during the development of the Trust Strategy 2025-30.
The 2024/25 survey programme will include the continuous surveys and various planned projects, ensuring incorporation of the Trust priorities and the Patient and Public Involvement strategic objectives. Key survey results and themes will continue to be reported as part of the Trust’s quality and assurance reporting channels, with the monthly PTS FFT figures reported to NHS England.
Planned survey projects 2024/25
- Planned projects to be undertaken during 2024/25 will relate to; the experience of our younger patients, complaints handling, advanced practice team, the complaints handling process, maternity care, mental health, and the implementation of the Patient Safety Incident Response Framework.
- The survey team will also be involved in the facilitation of an urgent care hub survey and the ongoing the Trust Strategy 2025-30 development.
Quality Governance Committee Assurance
Strategic Goals
- Goal 2: Provide Outstanding Quality of Care and Performance
Strategy Overview Areas
- Clinical Strategy
- Research and Innovation Strategy
- Quality Improvement Strategy
- Quality Account Priorities
Strategic Risks and Risk Overview Areas
- SR2: Failure to achieve continuous quality improvements and high quality care
- Clinical and Patient Safety
- Safeguarding
- Infection, Prevention and Control
- Estates
- Medical Devices
- Medicines Management
Key Change Initiatives
- CQC Improvement Plan
- Medicines Management Programme
- QI Faculty Development
- PAS Oversight Framework
Key Performance Indicators
- SI number, harm and actions
- IPC audit compliance
- Safeguarding compliance
- PAS metrics
- Drug audits and incidents
- Complaint metrics
- Fire and first aid compliance
- Clinical Quality Indicators
Key Independent Assurance Mechanisms
- Regulatory inspection reports
- Internal audit reports
- Healthwatch opinion
- Independent reviews
- Benchmarking
Sub-Group Structure

Compliance and Risk Group
- Patient Safety Group
- Clinical Best Practice Group
- Medicines Management Group
- Safeguarding Group
- Infection, Prevention and Control Group
- Patient Experience and Engagement Group
- Medical Devices Group
- External Provider Assurance Group
